

Epalrestat is a carboxylic acid derivative and a noncompetitive and reversible aldose reductase inhibitor used for the treatment of diabetic neuropathy, which is one of the most common long-term complications in patients with diabetes mellitus. The structure of epalrestat is showed in Figure 1.
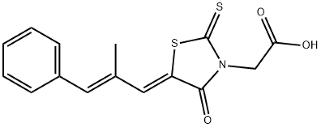
Fig. 1 Structure of epalrestat
Function of epalrestat in the treatment of diabetic neuropathy
- Introduction of diabetic neuropathy
Diabetic neuropathy is nerve damage that is caused by diabetes. Over time, high blood glucose levels, also called blood sugar, and high levels of fats, such as triglycerides, in the blood from diabetes can damage your nerves. Symptoms depend on which type of diabetic neuropathy you have.
Four main types of neuropathy can impact on the nervous system including:
- Peripheral symmetric neuropathy: This affects the feet and hands. It is the most common form of diabetic neuropathy.
- Thoracic and lumbar root, or proximal, neuropathy: This damages nerves along a specific distribution in the body, such as the chest wall or legs.
- Mononeuropathies: These can affect any individual nerve.
- Autonomic neuropathy: This occurs in the nerves that control involuntary functions of the body, such as digestion, urination, or heart rate.
The types of is showed in figure 2[1].

Fig. 2 Types of diabetic neuropathy
Diabetic neuropathy is one of the most common long-term complications in patients with diabetes mellitus, with a prevalence of 60-70% in the United States. Treatment options include antidepressants, anticonvulsants, tramadol, and capsaicin. These agents are modestly effective for symptomatic relief, but they do not affect the underlying pathology nor do they slow progression of the disease.
Epalrestat is an aldose reductase inhibitor that is approved for the improvement of subjective neuropathy symptoms, abnormality of vibration sense, and abnormal changes in heartbeat associated with diabetic peripheral neuropathy.
- Mechanism of action
The sorbitol (polyol) metabolic pathway, an alternative glucose reduction pathway involving the enzymes aldose reductase and sorbitol dehydrogenase, is thought to be activated by hyperglycaemic conditions. Intracellular accumulation of sorbitol during hyperglycaemia is considered to be at least partially responsible for the pathogenesis of late-onset complications of diabetes mellitus.
Epalrestat, an uncompetitive aldose reductase inhibitor, significantly reduces intracellular sorbitol accumulation in sciatic nerve, erythrocytes and ocular tissues from animal models, and in erythrocytes in humans, with diabetes mellitus, without affecting glucose levels. Epalrestat also increased sodium-dependent myoinositol uptake into sciatic nerve tissue in rats and skin fibroblasts from patients with diabetes, and attenuated nerve conduction velocity and retinal changes commonly seen in patients with diabetic neuropathy and retinopathy, respectively.